Imaging & data requirements
How to acquire the CT/CBCT and dental data we need for accurate orthognathic planning — our requirements from your side, on one printable sheet.
What Orthognathic Surgery Does
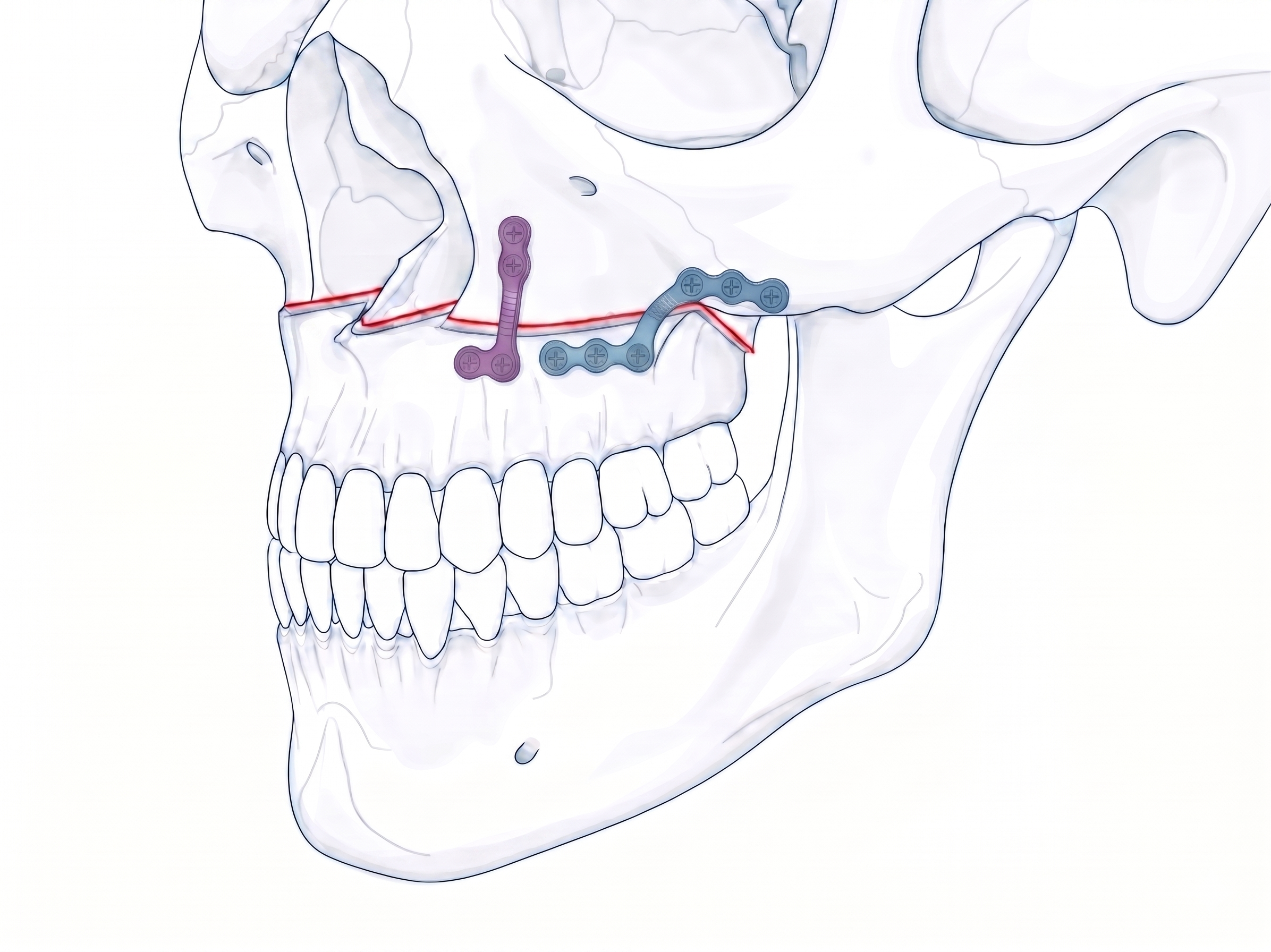
Orthognathic surgery repositions the upper jaw, the lower jaw, or both, to correct skeletal discrepancies that affect occlusion, breathing, chewing, and facial balance. The bones are cut along defined anatomical lines, moved into a planned position, and stabilized with titanium plates while they heal.
What sets the procedure apart is its reference frame. Most bone surgery is guided by the bone itself. Here, the destination is set by the teeth — the final occlusion is planned first, and the skeletal movements are derived from where the teeth need to go.
- Advancement
- the bone moves forward
- Setback
- the bone moves backward
- Impaction
- the bone moves upward
- Lowering
- the bone moves downward
- Rotation
- pitch, yaw, or roll change
- Translation
- lateral shift to correct asymmetry
Le Fort I, BSSO, Genioplasty
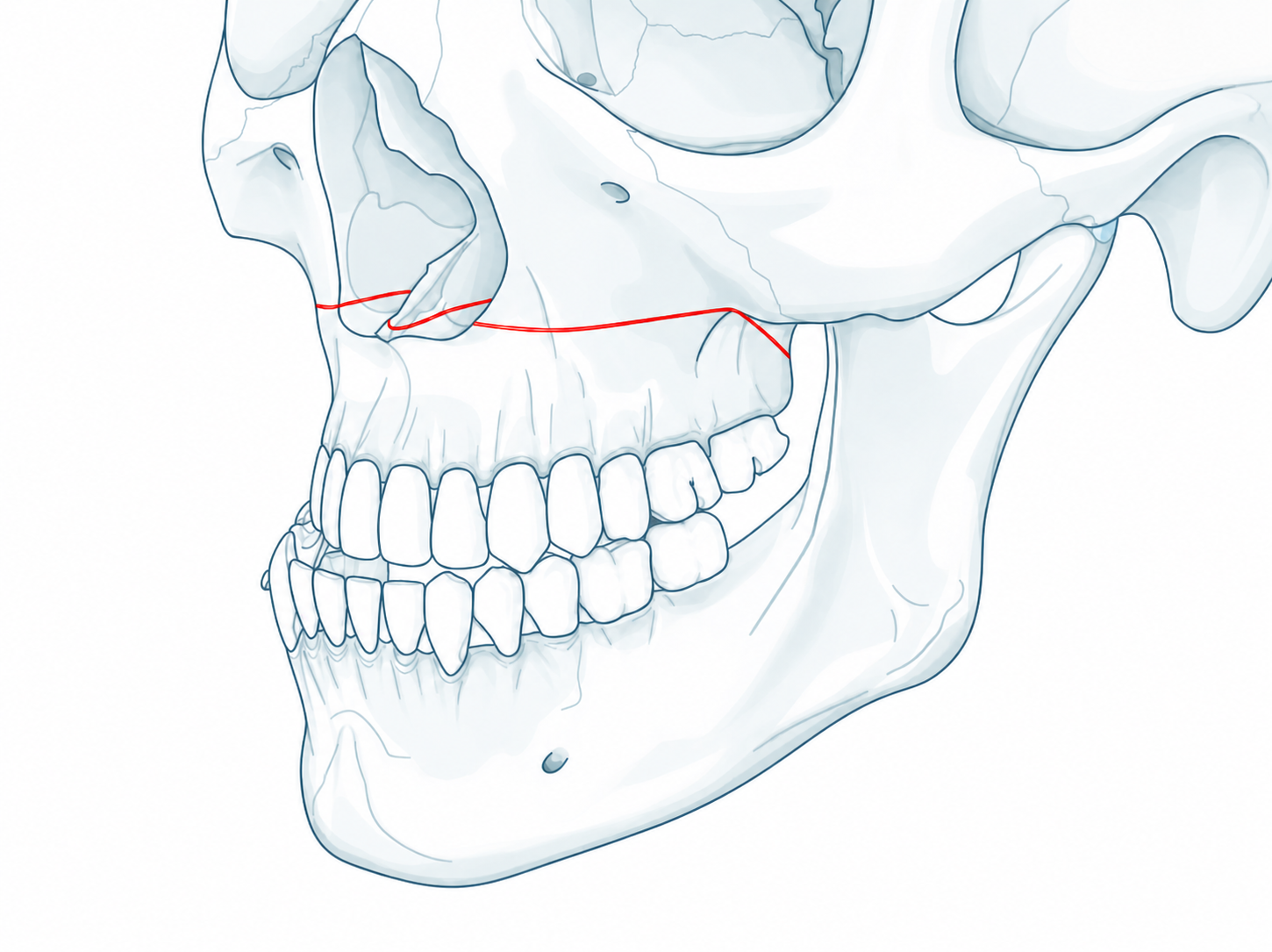
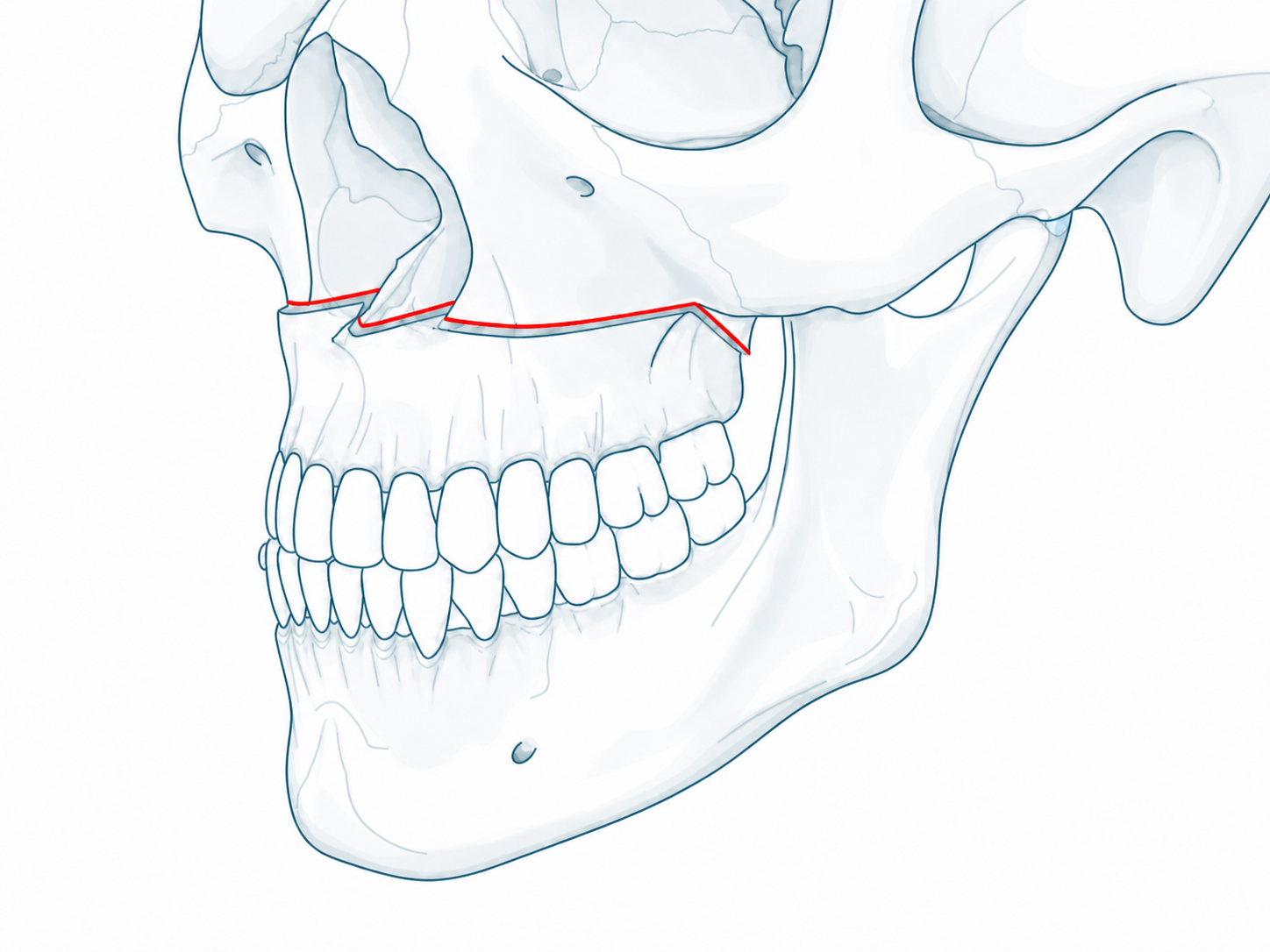
Three osteotomies form the building blocks of orthognathic surgery. They are performed alone or in combination depending on the diagnosis.
A horizontal osteotomy through the maxilla, passing above the tooth roots and below the orbital floor. Once separated from the midface, the maxilla can be advanced, set back, impacted, lowered, or rotated. A sagittal split through the palate also allows transverse expansion of the upper arch.
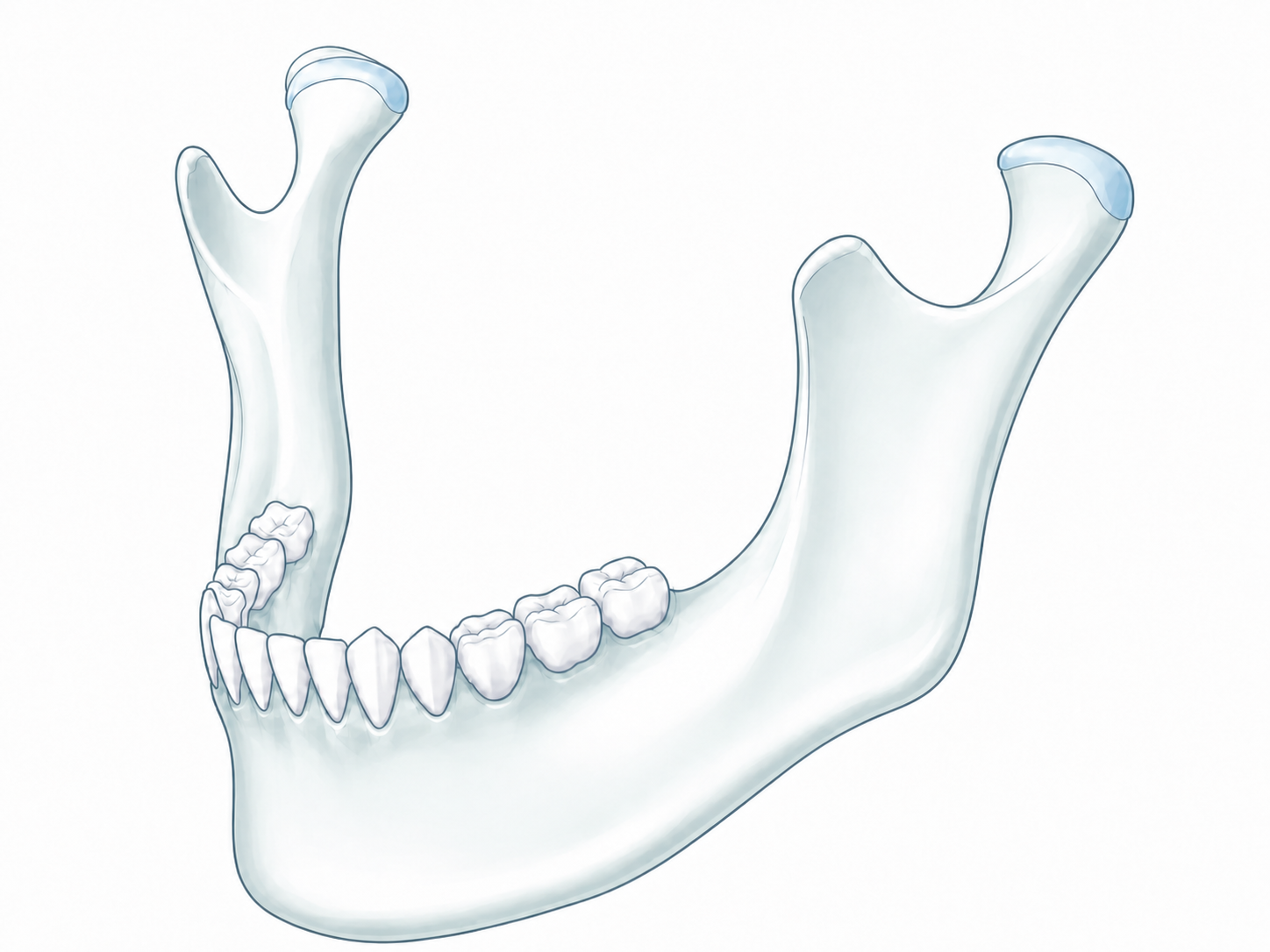
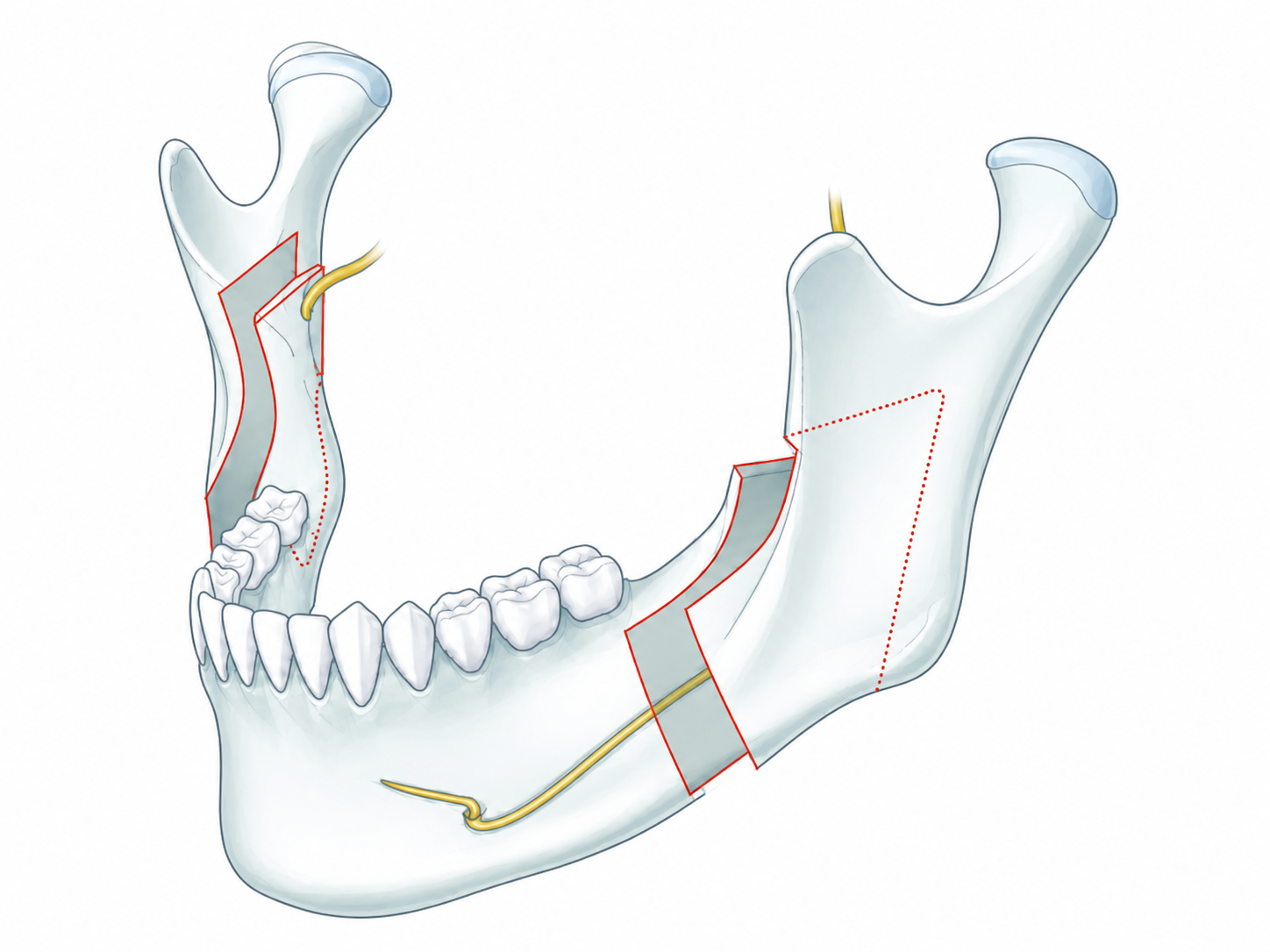
The lower jaw is split lengthwise through each ramus. The cut starts on the inner surface behind the last molar, then runs forward through the outer cortex, separating the jaw into two overlapping parts. The tooth-bearing part slides forward or backward into the planned position while the joint-bearing part stays put. The inferior alveolar nerve, which supplies feeling to the lower lip and chin, runs inside the bone; the split is planned around it so the nerve is released into the moving part and stays intact, and the broad bony overlap gives a stable surface for healing and fixation.
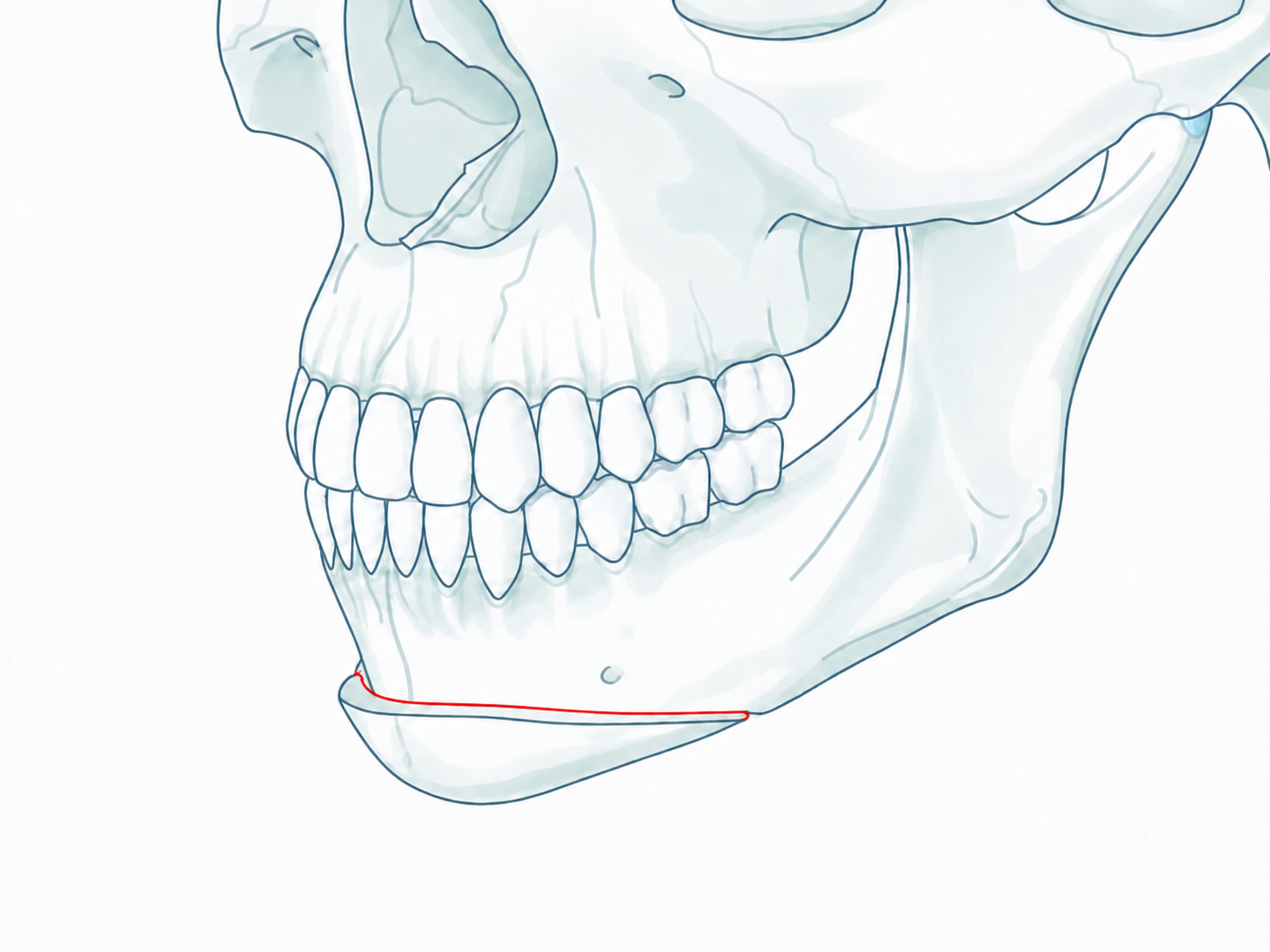
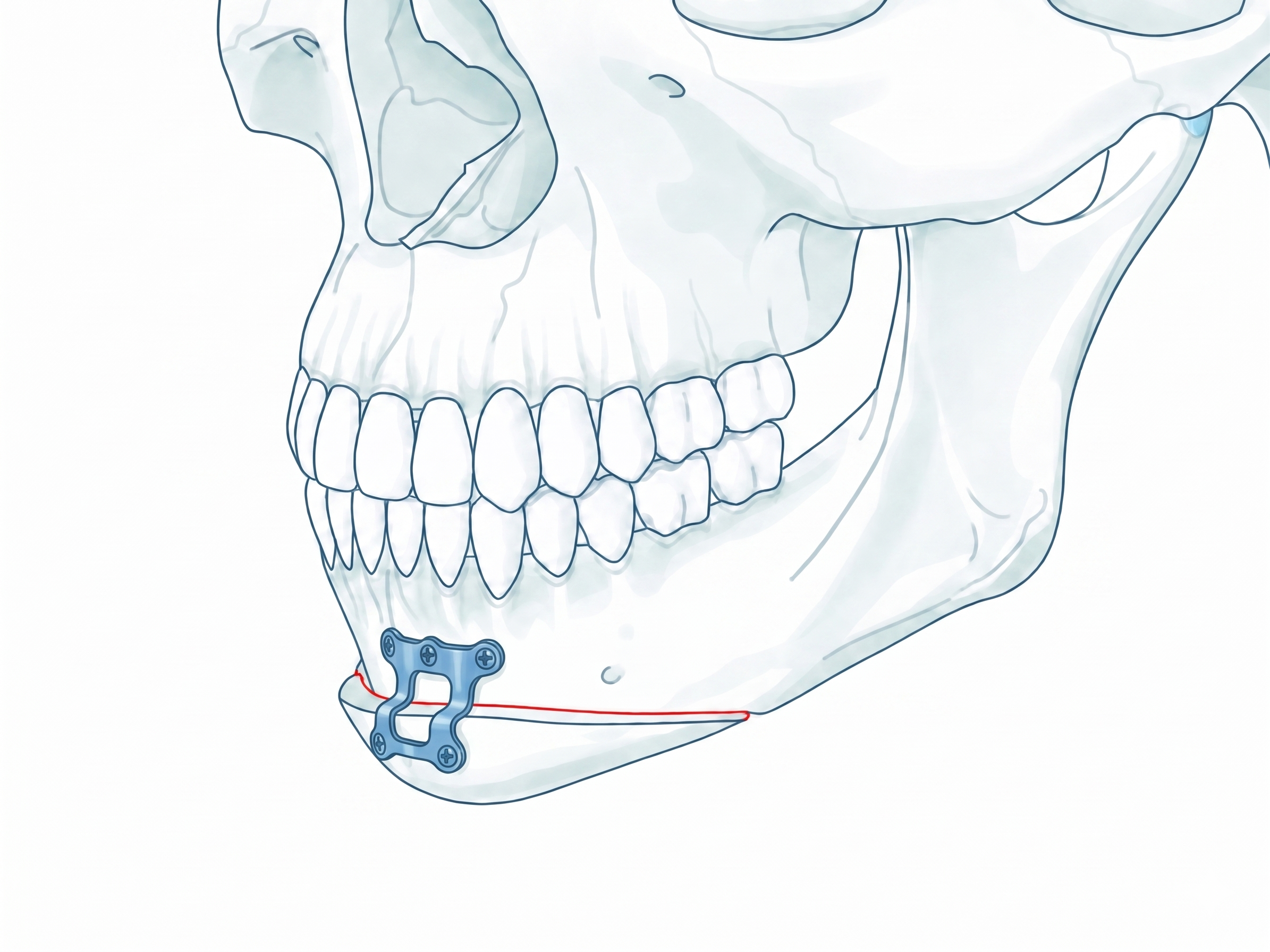
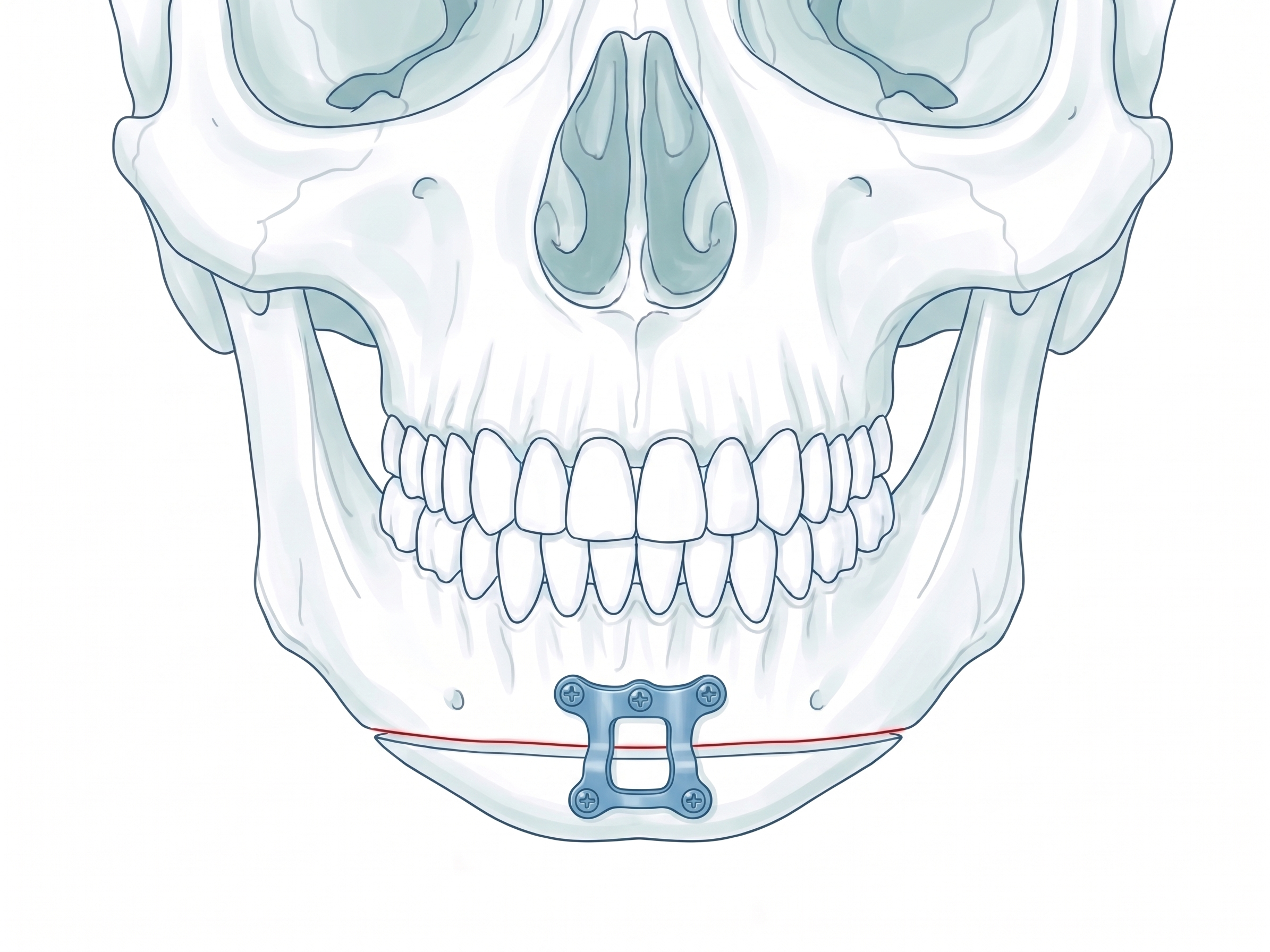
A horizontal osteotomy through the chin, made below the path of the mental nerve. The freed chin can move forward, backward, vertically, or laterally, and is most often combined with maxillary or mandibular surgery to refine facial balance and correct asymmetry.
Occlusion First
Before any bone is moved, the final bite is constructed virtually. Intraoral scans of the upper and lower dental arches are imported into the planning software and articulated into the ideal occlusal relationship — exactly as the teeth should meet after surgery.
This planned occlusion becomes the fixed reference of the entire case. Every skeletal movement — maxillary advancement, mandibular rotation, vertical correction, midline alignment — is back-calculated from where the teeth need to be. The dentition is the anchor; the bone is the variable.
Carrying the plan into surgery
The jaw movements are worked out in 3D on the computer. During the operation, that exact plan has to be reproduced on the patient so the bones end up where they were planned. This can be done in two ways.
Occlusal splint
The splint carries the plan directly. An occlusal splint is 3D-printed from the digital plan; during surgery the teeth are wired into it to reproduce the exact planned bite, and the bones are then fixed with titanium plates.
Custom titanium plates
Custom titanium plates carry the plan directly. Patient-specific cutting guides set where the bone is cut, and each plate fits only the planned position, so the bone is held exactly where it was designed to be, often without a separate splint.
Submit a case, receive a plan.
Send the patient's CT and dental scan through our secure channel. A planning proposal is typically returned within 2–5 working days, case-dependent.