Orthognathic surgery
Jaw repositioning plates
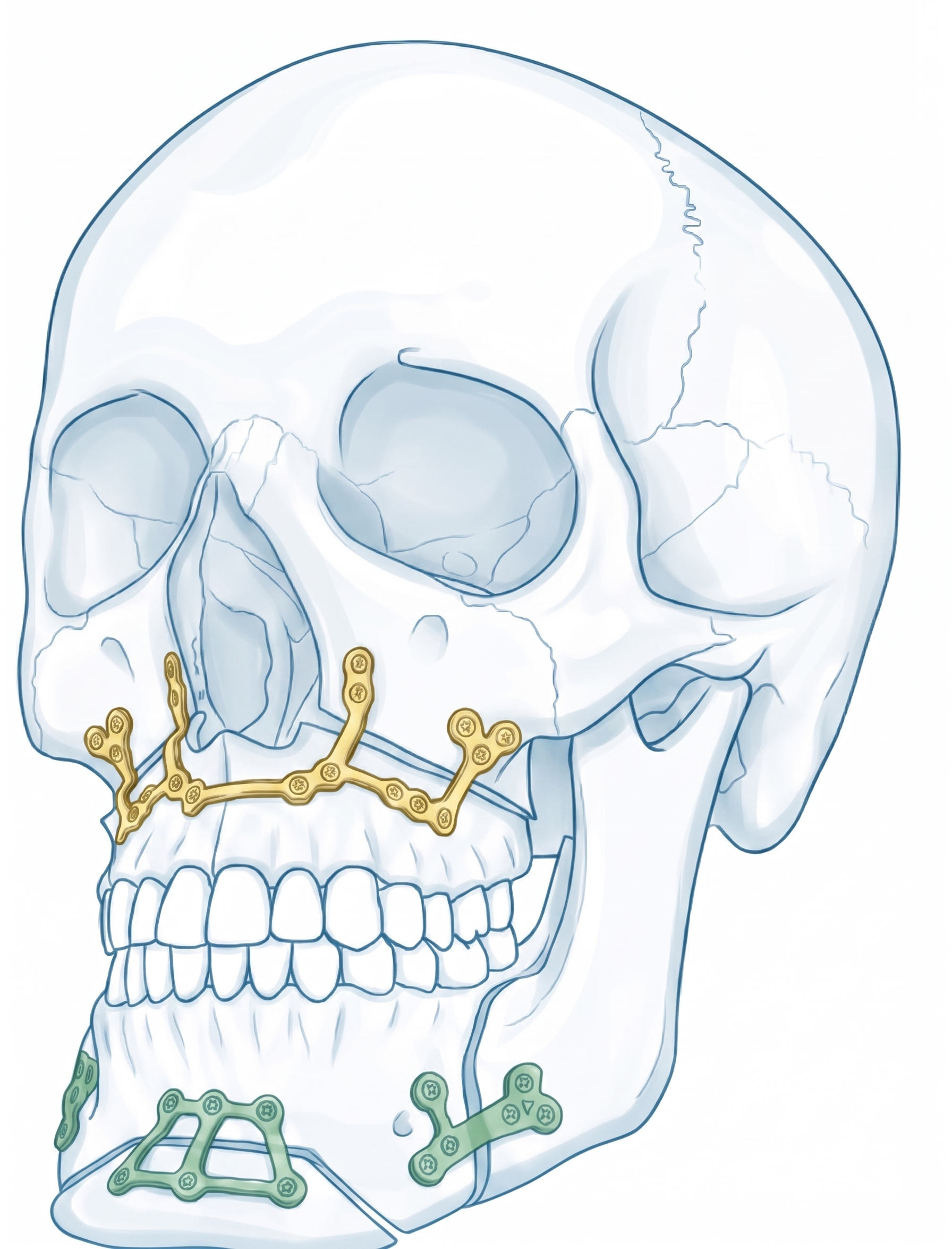
For Le Fort I, BSSO, or bimaxillary cases, plates are designed after the final occlusion and skeletal movement have been defined. The plate links the mobilized segment to the stable skeleton and helps transfer the virtual jaw position.
Screw holes can be coordinated with osteotomy lines, tooth roots, maxillary sinus anatomy, and planned guide positions.